
Diet Review Series: Keto
From Director of Health Alex Maples
Because carbs are the root of all evil… right?
The keto diet has cooled in recent years, but for much of the past decade it was the “it” diet in the weight-loss space.
Keto originated in the 1920s as a medical intervention for epilepsy, especially in children. Doctors noticed that, while fasting dramatically decreased seizure frequency, it was not a viable long-term strategy for growing kids. Dr. Russell Wilder at the Mayo Clinic hypothesized that ketosis might be responsible for the improvement and proposed a diet designed to mimic fasting’s metabolic state while still providing adequate calories.
The original therapeutic ketogenic diet was roughly 80%-90% fat, with carefully controlled protein and only trace carbohydrates. It was highly effective for epilepsy and became a go-to treatment at the time, before fading when anticonvulsant medications arrived in the 1930s and offered a far more convenient option for families. Keto persisted in medication-resistant epilepsy (and a handful of other neurologic applications), but largely disappeared from public view.
That changed in the 1970s when Dr. Robert Atkins popularized low-carbohydrate dieting for weight loss and metabolic health in Dr. Atkins’ Diet Revolution. His thesis ran counter to prevailing wisdom, which held that dietary fat drove cardiovascular disease and should be avoided. (Even in the pre-internet era, contrarian ideas had their appeal.) Through the 70s and 80s, Atkins simmered in the background while the mainstream food industry pivoted to low-fat everything.
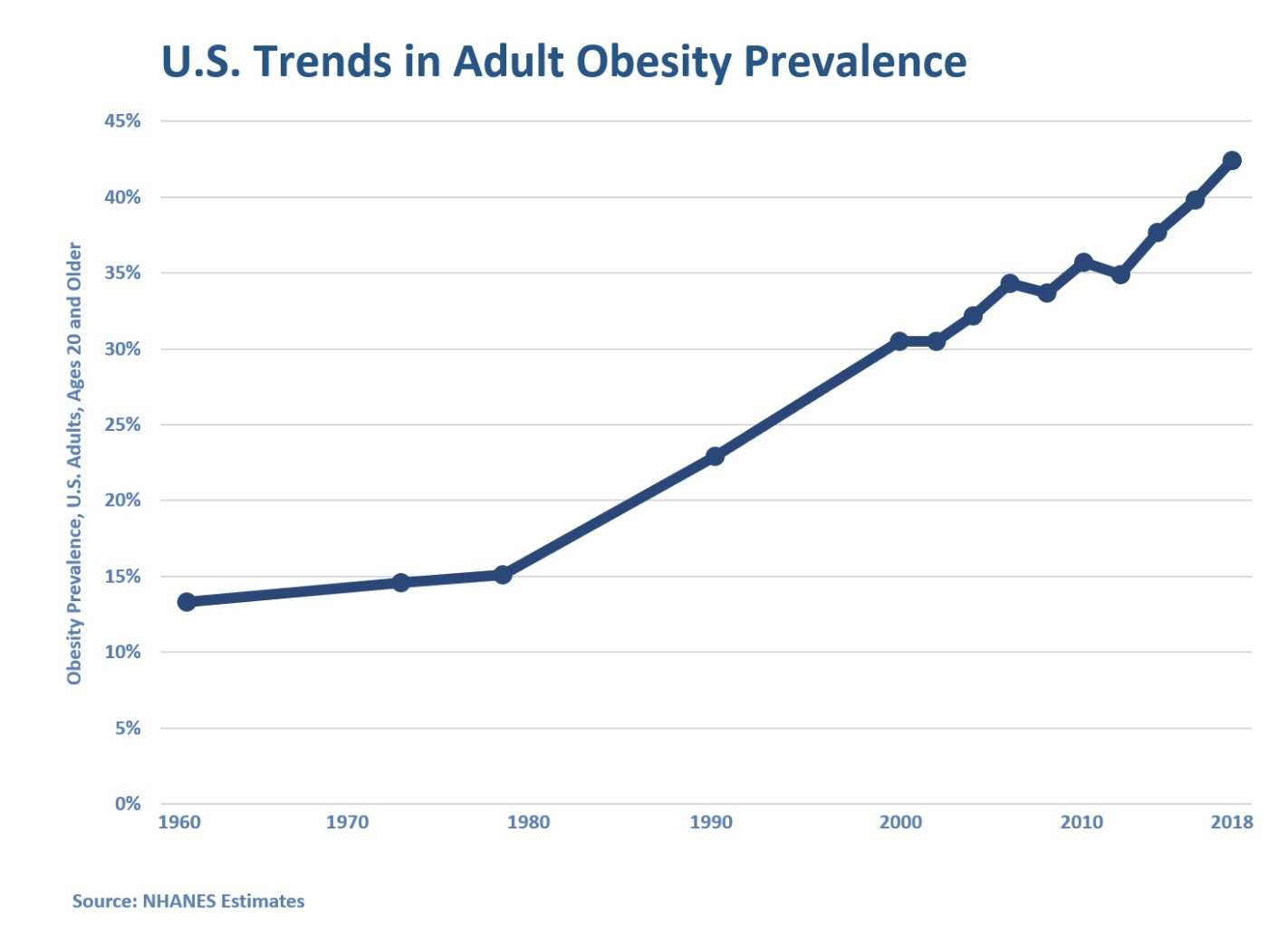
Meanwhile, the obesity epidemic was snowballing. By the mid-to-late 90s, public frustration was boiling over. People felt they’d done everything “right”: high-carb, low-fat, lots of jogging and aerobics, yet they were heavier than ever. When Atkins re-released his book in the late 1990s, it said what many people were already thinking: this isn’t working. It went nuclear, selling over 10 million copies and spending multiple years on the New York Times bestseller list in the late 1990s and early 2000s.
The narrative was simple and provocative. You’ve been lied to, fat isn’t what’s making you fat, carbs are. Here is what to do instead.
Atkins’ approach wasn’t “no carbs forever.” It was a structured reset with four phases.
Phase 1: Induction
Duration: At least 2 weeks
Goal: Initiate weight loss, reduce appetite
<20g of carbohydrates per day from leafy greens
Moderate protein
Higher fat by default
Phase 2: Ongoing Weight Loss (OWL)
Duration: Highly individualized
Goal: Continue losing fat and find carb tolerance
Gradually increase carb intake by 5g/week
Begin to introduce nuts, seeds, berries, and small amounts of higher carb foods
Seek maximum carb intake while still losing weight
Phase 3: Pre-maintenance
Duration: Highly individualized
Goal: Slow weight loss and find maintenance
Increase carb intake by 10g/week
Expand food variety
Identify carb intake for maintenance
Phase 4: Maintenance
Duration: Indefinite
Goal: Maintain weight loss with a less restricted eating pattern
Unlike the caricature of Atkins, the actual diet was a far more nuanced intervention aimed at restoring appetite control and gradually reintroducing carbohydrates. In many ways, that made it a better long-term framework than what it eventually evolved into. But nuance doesn’t go viral.
The early phases produced rapid, visible feedback. But, maintenance required self-regulation without dramatic reinforcement.
As often happens when structure loosens, things slip and weight regain follows. The hardest part of most diets isn’t losing weight, it’s maintaining it. Gritting your teeth and following rigid rules is often easier than learning to moderate when the lines get blurry.
Add in a slew of Atkins-branded processed foods, and the problems multiplied. The diet that was built around whole foods began selling packaged snack bars, and its credibility took a hit.
“Biohacking,” butter coffee, and the rise of KETO 4 EVA
Like a phoenix from the ashes, low carb rose again in a new form. This time with less nuance and more buzzwords.
Ketones! Autophagy! Mitochondrial Biogenesis! Epigenetics!
The early 2010s saw the rise of direct-to-consumer health information and the proliferation of long-form podcasts. With it came keto’s resurgence. The narrative shifted from losing weight to optimizing your biology.
Figures like Peter Attia (rigorously) and Dave Asprey (less so) began discussing ketosis as a powerful metabolic tool, framing it as a path to metabolic optimization.
Arthritis: Ketosis
Eczema: Ketosis
Brain Fog: Ketosis
Depression: Ketosis
ED: Ketosis
Some of these claims had plausible mechanisms. Others raced ahead of the human data.
This time around, the tools to make it data-driven were there: ketone breath meters, urine strips, blood ketone testing. Suddenly there was a quantifiable target outside of calorie counting, a clear biochemical definition of “doing it right.”
Even the framing reinforced the simplicity. Gary Taubes’ book was titled Good Calories, Bad Calories.
Add in highly visible podcasters amplifying expansive claims about ketosis, and you had a recipe for virality.
How Keto Works
In its strict therapeutic form, the ketogenic diet used for epilepsy can reach 80%-90% of calories from fat, with carefully controlled protein and minimal carbohydrates.
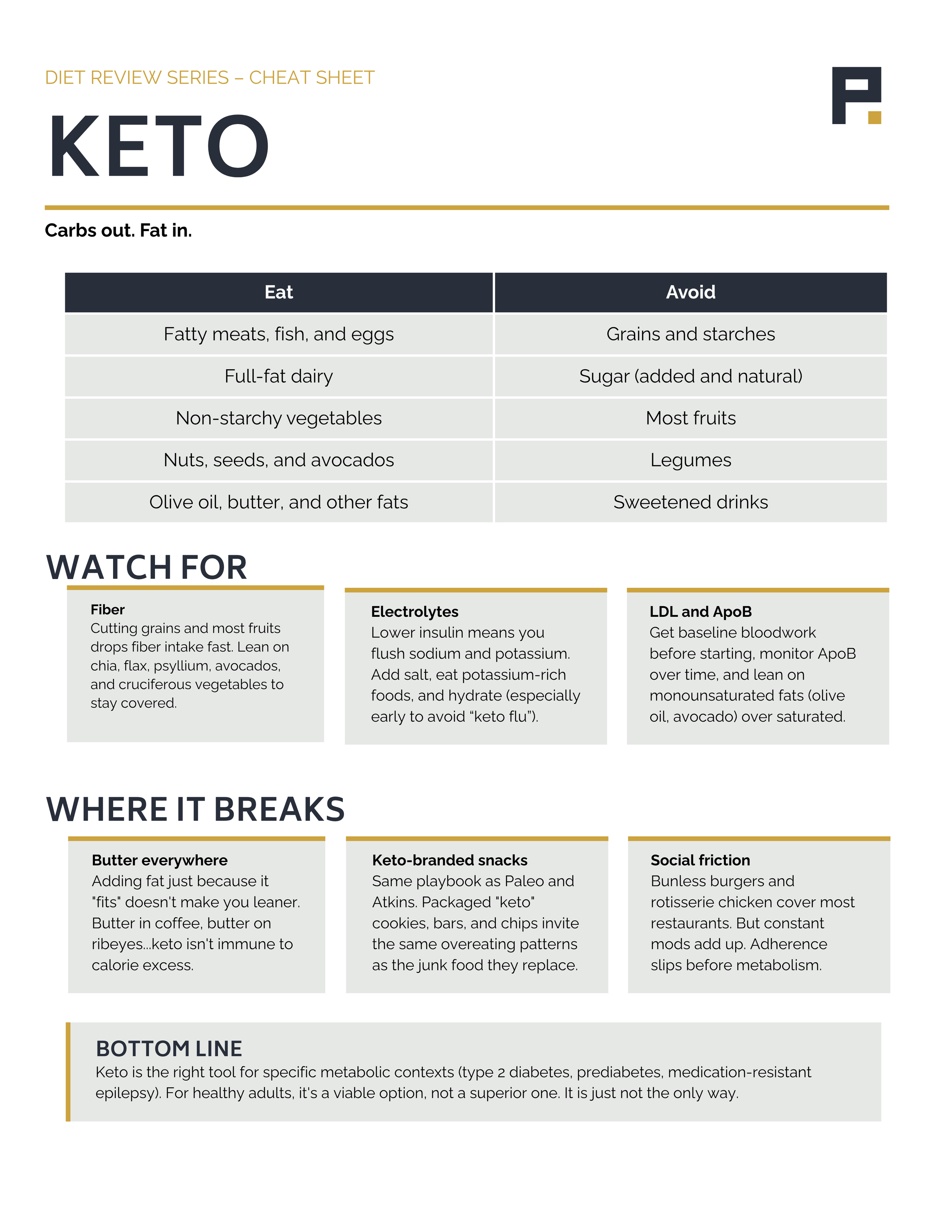
In practice, lifestyle keto typically looks like high fat, moderate protein, and very low carbohydrate (often under 50g per day) with the goal of sustaining nutritional ketosis.
Potential Nutrient Gaps
Keto is not inherently nutrient-deficient, but it does remove several food groups that commonly provide fiber and key micronutrients. Without deliberate attention to vegetables, minerals, and seafood, gaps are possible.
Fiber: One of the most common shortfalls on a keto diet is fiber, especially if intake of non-starchy vegetables is low. There are solid low-carb sources such as chia seeds, flax, psyllium husk, avocados, and cruciferous vegetables, but they require intentional inclusion.
Sodium and Potassium: While not inherently lacking, carbohydrate restriction lowers insulin levels, which increases sodium excretion by the kidneys. Water, sodium, and potassium losses can contribute to fatigue, headaches, and the so-called “keto flu.” Being intentional about electrolyte intake, especially early in the diet, is important.
A Note on LDL Cholesterol
One of the most debated aspects of the keto diet is its effect on LDL cholesterol, and specifically the number of ApoB-containing particles in your blood. ApoB (apolipoprotein B) is the protein on the surface of LDL and related particles, and counting it is increasingly viewed as a more precise measure of cardiovascular risk than LDL cholesterol alone. The relationship between elevated ApoB and cardiovascular risk is well established.
Keto doesn’t cause LDL to rise in everyone, but for some it increases LDL and ApoB substantially. ApoB monitoring is the key marker to watch if you’re doing a long-term keto diet.
It’s worth noting that saturated fat intake generally raises LDL and ApoB. Limiting saturated fat and prioritizing monounsaturated fats such as olive oil and avocado may help mitigate that response.
How We Break It (Common Failure Modes)
Keto is largely built around the idea that dramatically reducing carbohydrate intake decreases appetite and, in turn, total caloric intake. For many people, this is true.
But keto is not immune to calorie excess. If you intentionally add large amounts of fat (butter in coffee, butter on ribeyes…) you can override appetite regulation. It’s possible to do this without exceeding your energy needs, but it becomes less likely as energy density rises.
Like any dietary pattern, sustained calorie surplus leads to weight gain. And, as discussed earlier, extremely high saturated fat intake may also negatively affect LDL and ApoB levels.
That said, keto deserves credit here. When adhered to strictly, if the foods are boring and engineered to tamp down your appetite, it’s harder to overeat.
Sustainability Factor
This is where the appetite-control advantage really gets put to the test.
Is keto sustainable? For some people, yes. For others, much less so.
Keto is a highly restrictive diet. Removing most carbohydrate-rich foods significantly reduces variety. Some people thrive within that structure; others find it difficult to sustain.
From a restaurant and convenience standpoint, there are usually workable options: a bunless burger, a salad with added protein, and rotisserie chicken. But long-term social flexibility matters, and for many people the constant modification becomes friction.
The Final Verdict
There are clear contexts where the keto diet has distinct advantages.
If you have type 2 diabetes or prediabetes, carbohydrate restriction can significantly reduce blood glucose and A1C. These conditions are rooted in insulin resistance and impaired carbohydrate metabolism. In that context, removing carbohydrates can produce meaningful clinical improvements.
In its original therapeutic role, keto remains an effective treatment for medication-resistant epilepsy and certain neurological conditions.
But if you already have healthy blood sugar regulation, there appears to be little added benefit (and potentially some downside from an athletic performance perspective) to removing carbohydrates entirely.
The keto diet is not the “optimal human diet.” It may, however, be the optimal diet in certain metabolic contexts, and that makes it valuable.
If you choose to follow a keto diet, monitor LDL and ApoB, prioritize fiber and micronutrients, and pay attention to fat quality. Done thoughtfully, it can be an effective way to manage appetite and support metabolic health. It’s just not the only way.
New to the Diet Review Series? Start with Setting the Table — it lays out the fat-loss lens we run every diet through.